
Alfamino® HMO
Hypoallergenic amino acid-based formula (AAF) with 2 HMO (2'-FL and LNnT) for effective first-line symptom relief in infants and young children with severe forms of CMPA, Multiple Food Protein Allergy and other conditions requiring an AAF.
A sole source of nutrition from birth to 12 months of age. Supplement in combination with age-appropriate complementary foods from around 6 months of age.
Advancing the
Management of
Cow’s Milk
Protein Allergy
Preparing Alfamino® HMO is very similar to how you prepare standard infant formula. The step-by-step instructions on how to prepare Alfamino® HMO are:

STEP 1 Wash hands before preparation.

STEP 2 Wash hands before preparation.

STEP 3 Boil for 5 min. Leave covered until use.

STEP 4 Boil drinking water for 5 min, allow to cool.

STEP 5 Pour exact amount of lukewarm water into bottle.

STEP 6 Add exact number of level scoops for age of babyas per feeding table on tin.

STEP 7 Shake bottle until powder fully dissolved. Use immediately and do not keep unfinished bottle, discard contents.

STEP 8 Close tin tightly after each use and store in a cool, dry place. Must be used within 3 weeks of opening.
WARNING “Unboiled water, unsterilsed bottles or incorrect dilution can make your baby ill. Incorrect storage, handling, preparation and feeding can also lead to adverse effects. Follow instructions carefully. ”
| AGE | QTY PER MEAL (ML) | QTY PER MEAL (SCOOPS) | MEALS PER DAY |
|---|---|---|---|
|
1-2 weeks
|
90
|
3
|
6
|
|
3-4 weeks
|
120
|
4
|
7
|
|
2nd month
|
150
|
5
|
5
|
|
3-4 months
|
180
|
6
|
5
|
|
5-6 months
|
210
|
7
|
5
|
|
From 5th (7th) month**
|
210
|
7
|
3-4
|
Glucose syrup, vegetable oils (sunflower, rapeseed, structured palm oil), amino acids, MCT, starch, minerals (calcium glycerophosphate, potassium chloride, sodium citrate, calcium citrate, potassium citrate, sodium phosphate, magnesium oxide, ferrous sulphate, zinc sulphate, copper sulphate, potassium iodide, manganese sulphate, sodium selenate), emulsifier (E472c), Fibre(2'-Fucosyllactose, Lacto-N-Neotetraose), mortierella alpina oil (ARA), choline bitartrate, Schizochytrium sp. oil (DHA), vitamins (C, E, niacin, pantothenic acid, riboflavin, A, thiamin, B6, folic acid, K, D, biotin, B12), acidity regulator (E330), taurine, inositol, L-Carnitine.

Osmolarity = 299 mOsm/l
NE = Niacin equivalent
DFE = Dietary folate equivalent
DHA = Docosahexaenoic acid
ARA = Arachidonic acid
- Proven hypoallergenic with a tolerance of 100% in infants and children with cow’s milk protein allergy (CMPA)1
- Supports growth and is well tolerated2-4 including in severe forms of CMPA4,5
- Provides immune enhancing properties with the addition of 2 HMO (2’-FL and LNnT†), to support the growth of beneficial bacteria and the production of important short chain fatty acids4
- Reduces the risk of common respiratory-tract infections as well as medication use in infants with CMPA through the addition of 2’-FL and LNnT† to formula6
- Inspired by breastmilk with structured lipids (40% in sn-2 position) - associated with higher bone mineral density and better stool consistency7-8
- Designed to support tolerance and absorption with 24.4% MCT9-13
- Promotes acceptance/compliance with preferred taste over some other amino-acid-based formula14
†LNnT = Lacto-N-neotetraose; 2’-FL= 2’-Fucosyllactose; HMO = Human milk oligosaccharides; MCT, Medium chain triglycerides; HMO, Human milk oligosaccharides.
Immune-Nurturing Benefits
CMPA is an immune-mediated condition. It is associated with gut microbiota dysbiosis, which impacts immune system maturation and leaves infants at an increased risk of infections and future allergies.15 Alfamino® HMO contains lactose, as well as 2’-fucosyllactose (2’-FL) and lacto-N-neotetraose (LNnT). 2FL and LNnT are two significant human milk oligosaccharides (HMO) that are structurally identical to those found in breastmilk.16
HMO are bioactive components that support the infants in the following ways.17,18




Reducing Infections and Medication Use
Infants fed formula with 2’-FL and LNnT† had fewer upper and lower respiratory tract infections6
Infants fed formula with 2’-FL and LNnT† had lower antibiotic and antipyretic use6,19
Patient Case Example For Alfamino® HMO
NAME & AGE
Sophia, 6 months old
DIAGNOSIS
Sever Cow’s Milk Protein Allergy
DIETARY MANAGEMENT
Alfamino® HMO

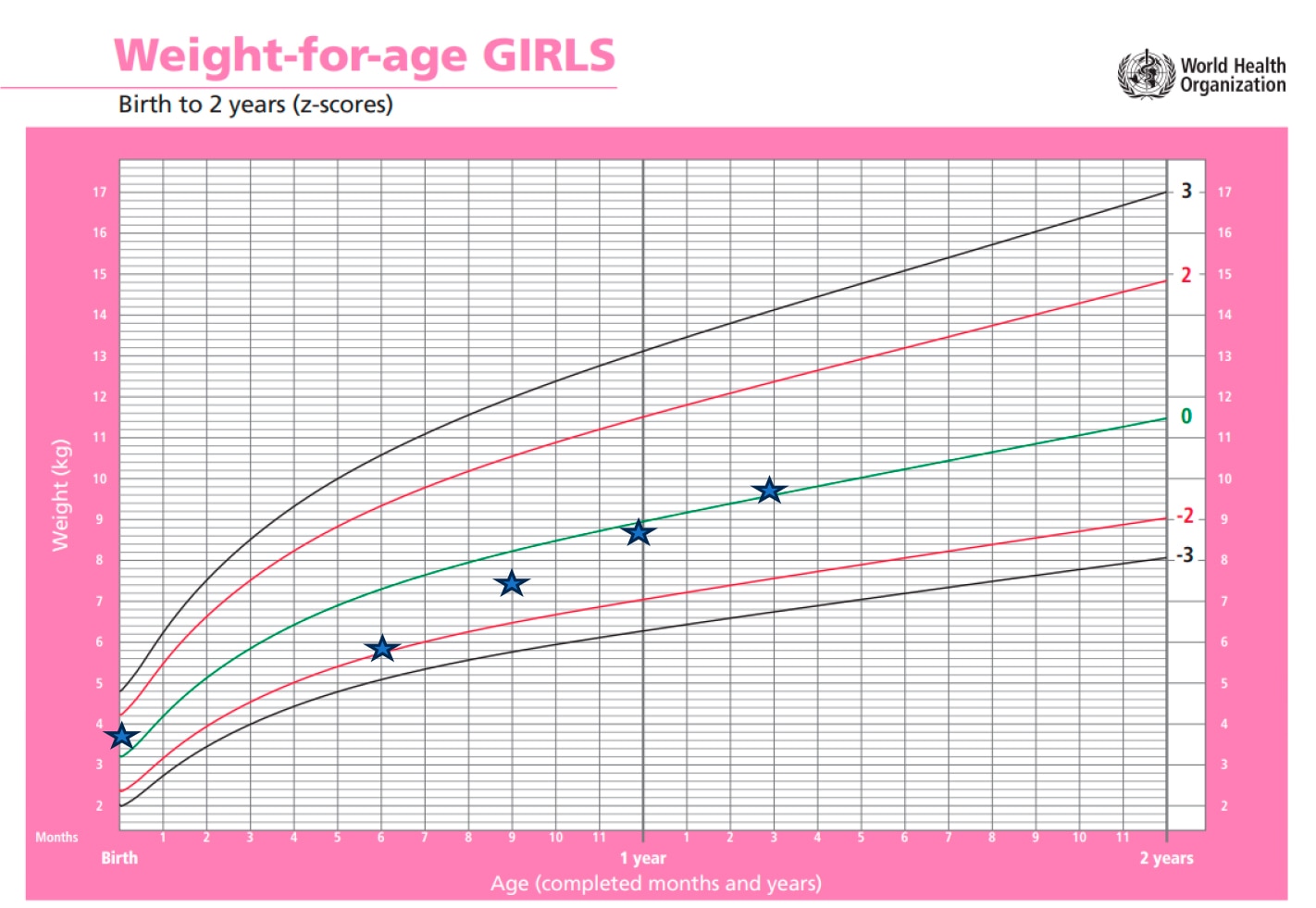
Case presentation: SOPHIA
Sophia, a 6-month-old girl – with severe atopic dermatitis and faltering growth – she had not achieved symptom resolution on an extensively hydrolyzed formula (eHF). She had been exclusively breastfed for the first 4 months and had dry skin from birth, which worsened when she started standard infant formula. She was prescribed emollients and was changed to an eHF at 5-months by her general practitioner (who suspected allergy). This resulted in some improvement, but she continued to have poor growth. She was referred to a dermatologist for assessment.
Atopic Dermatitis (AD) with Faltering Growth (fall of 1 SD from birth to 6 months – birth weight 3.7kg weight-for-age z-score (WAZ) 0 = normal, at 6 months weight 5.7kg, (WAZ -2), and cow’s milk protein allergy (CMPA).
The dermatologist prescribed topical corticosteroids and referred her to a dietician.
The dietician recommended changing from the eHF to an amino-acid-based formula (AAF) (Alfamino® HMO) due to her poor growth and severe AD and proposed a review at 8 months of age. The dietician also provided advice on dairy free complementary feeding.
Sophia’s weight had improved to 7.2kg, WAZ close to 0 at 8 months. Her skin was much better but mum reported flare-ups with certain foods – including wheat and fish, so she was excluding these from Sophia’s diet, along with dairy and soy. They agreed to continue the current diet until her next review when they would consider food challenges.
Her dermatologist had advised a reduction in her topical steroids and to continue with emollients.
On review she was growing well (8.7kg, WAZ 0 = normal) and taking ~500ml/day of Alfamino HMO. She was eating well and had a varied diet, although mum was still excluding some foods (dairy, soy and fish). She was now tolerating some wheat-based products. The dietician started dairy reintroduction using the milk ladder at home, but mum reported skin flare-up following the fresh milk challenge. Sophia seemed to tolerate small amounts of soy. The dietician advised that she continue to encourage all foods that were tolerated, excluding only fresh milk and fish for now. It was also suggested to gradually wean her off Alfamino HMO over a period of 1-2 months (while monitoring her weight). At her follow-up review (15 month), mum reported that Sophia had stopped Alfamino HMO and was taking a commercially available soy-based drink with added calcium. She was still avoiding fish and fresh milk, but Sophia now tolerated baked milk products. She was growing well with her WAZ now back to norma (WAZ = 0). She continued to be seen by the dermatologist, although her skin was also much improved.
Introducing Our Plant-Based Packaging Designed to Be Recyclable
Our plant based plastic is made from sugar cane which is a renewable resource unlike fossil based material. Additionally, we have ensured a lighter pigment colour to improve recyclability.

…of the plastic in the Alfamino lid and scoop combined are now made with plant-based materials (sugar cane) instead of fossil fuel-based materials.
How We Convert Sugar Cane to Plant Based Plastic
Curious to learn more about how our plant based plastics are typically made?


This is where the resin to make our plant based plastic comes from.

Alfamino® HMO FAQs
Answers to common questions
about
Alfamino® HMO.
The tin size of Alfamino HMO is 400g.
It is 4.4g – so 1 scoop of Alfamino® HMO is equal to 4.4g of powder.
Yes, Alfamino® HMO can be used for infants requiring enteral tube feeding. Instructions need to be followed according to local guidance as well as the patient’s individual nutritional management plan.
Alfamino® HMO is suitable for those following a halal or kosher diet. The protein used in Alfamino® HMO is based on 100% free amino acids. This formula meets the hypoallergenicity criteria of the American Academy of Pediatrics (AAP) and can be used for the dietary management of infants with CMPA.1
1. Nowak-Wegrzyn A, et al. Clin Pediatr. 2015.
Medium-chain triglycerides (MCT) are made up of a mixture of triacylglycerols consisting of saturated fatty acids with a chain length of 6–10 carbons.1-3 MCT are easily absorbed because they are relatively soluble in water.3 Consequently, they are hydrolyzed both faster and more completely than long-chain triglycerides (LCT), the faster action of pancreatic lipase being facilitated by their small molecular weight.3 These benefits appear to be useful for infants with an immature gut or those with intestinal failure.4 MCT therefore provide a rapid energy source.5 Adding MCT to formulas has been shown to be beneficial in severe fat malabsorption, such as intestinal failure.4 Alfaré® HMO, Alfamino® HMO and Alfamino® Junior HMO contain 40%, 24% and 24% respectively of MCT fats, which may support energy uptake in infants with severe gastrointestinal impairment (including infants with severe enteropathy affecting fat absorption related to CMPA).
1.Bach AC, & Babayan VK. Am J Clin Nutr. 1982;36(5):950-62.
2.Marten B, et al. Int Dairy J. 2006;16:1374-82.
3.Clegg ME. Int J Food Sci Nutr. 2010;61(7):653-79.
4.Delplanque B, et al. J Pediatr Gastroenterol Nutr. 2015;61(1):8-17.
5.Babayan VK. Lipids. 1987;22: 417-20.
The following conditions have been included in a practical evidence based guide1 on the use of AAF:
- • Failure on an extensively hydrolyzed formula (eHF)
- • Eosinophilic Esophagitis
- • Growth faltering, in particular with multisystem involvement (gastrointestinal tract/and or skin) and multiple food eliminations
- • Anaphylaxis
1.Meyer R, et al. J Allergy Clin Immunol Pract. 2018;6:383-99.
Alfamino® HMO is based on 100% free amino acids, contains 24% of it’s fat as medium-chain triglycerides (MCT) and is lactose free. These are important attributes for infants and children with severe forms of CMPA and also support those with severe gastrointestinal (GI) impairment. MCT are easily absorbed and are hydrolyzed both faster and more completely than long-chain triglycerides (LCT).1 This has been shown to be useful for infants with GI impairment.2 Meanwhile being lactose free supports those cases with secondary lactose intolerance.
1.Bach AC, & Babayan VK. Am J Clin Nutr. 1982;36(5):950-62.
2.Delplanque B, et al. J Pediatr Gastroenterol Nutr. 2015;61(1):8-17.
Differences in lipid composition between these formulas relate to the target population of the formulas. For example, gastrointestinal impairment, which can:
• occur in combination with CMPA symptoms: Alfaré® HMO is recommended
or
• occur in those with severe CMPA symptoms: Alfamino® HMO is recommended (or Alfamino® Junior HMO when the child is >1 year)
Alfaré® HMO, Alfamino® HMO and Alfamino® Junior HMO contain medium-chain triglycerides (MCT). MCT are easily absorbed, which is useful for infants with an immature gut or intestinal failure.1,2 Althéra® HMO does not contain MCT and is indicated, as first line management, for infants with CMPA.
In addition, only Alfamino® HMO and Alfamino® Junior HMO contain structured lipids, mimicking the composition and structure of palmitic acid in breastmilk, to facilitate fat and calcium absorption.2,3
Regardless of their lipid composition, the four formulas in the range, Althéra® HMO, Alfaré® HMO and Alfamino® HMO and Alfamino® Junior HMO are suitable for the management of CMPA.
They all contain the essential fatty acids linoleic acid (LA) and α-linolenic acid (ALA), as well as the long-chain polyunsaturated fatty acids (LCPUFA), arachidonic acid (ARA) and docosahexaenoic acid (DHA), which are important for brain and immune development.2
1. Bach AC, & Babayan VK. Am J Clin Nutr. 1982;36(5):950-62.
2. Delplanque B, et al. J Pediatr Gastroenterol Nutr. 2015;61(1):8-17.
3. Mazzocchi A, et al. Nutrients. 2018;10(5):567.
HMO structures are quite complex, and the replication of HMO (that are structurally identical, but not sourced from human milk) was not possible until recently.
That’s why formulas have often been supplemented with simpler oligosaccharides such as galacto-oligosaccharides (GOS), a (non-human) milk-derived oligosaccharide (enzymatically produced from galactose)1 or a plant-based variety, fructo-oligosaccharides (FOS) – not found in human breastmilk1,2.
Advances in biotechnology, after almost 30 years of research and development by Nestlé and their partners, enabled the production of HMO, including 2’fucosyllactose (2’-FL) and lacto-N-neotetraose (LNnT); now produced on an industrial scale to introduce into standard and specialty infant formulas. 2’-FL and LNnT in Nestlé formulas are structurally identical to two of the top 10 HMO in human milk.2
1.Sela D & Mills D. Trends Microbiol. 2010 July ; 18(7): 298–307.
2.Bode L, & Jantscher-Krenn E. Adv Nutr. 2012;3(3):383S-91S.
More than 200 HMO have been identified in breastmilk,1 with 2’fucosyllactose (2’-FL) and Lacto-N-neotetraose (LNnT) being among the 10 most abundant, accounting for more than 30% of all HMO.2 They are well studied and are considered to be safe for use in standard infant formula and in speciality infant formulas by the European Food Safety Authority (EFSA).3
The first clinical studies in healthy infants using standard infant formulas supplemented with 2’-FL and LNnT demonstrated their safety, supporting normal growth, with beneficial effects on immunity, gut microbiota development and the rate of some infections as well as the need for some medications.4-6 Clinical studies in infants with cow’s milk protein allergy (CMPA) showed that our specialty formulas containing 2’-FL and LNnT were hypoallergenic, supported normal growth, effectively alleviated CMPA symptoms, reduced the risk of infections and potentially the need for some medications,7 and positively shaped the gut microbiome.7-10
Infants with CMPA can now benefit from two of the most abundant HMO in human milk, 2’-FL and LNnT, which have been proven to nurture the infants’ immune system, addressing gut microbiota dysbiosis and reduce the risk of infections4-10 and potentially the need for some medications.7
1. Walsh C, et al. J Funct Foods. 2020;72:104074.
2.Azad MB, et al. J Nutr. 2018;148(11):1733-42.
3.EC No 258/97. EFSA J. 2015;13(7):4183.
4.Berger B, et al. mBio. 2020;11(2):e03196-19.
5.Puccio G, et al. J Pediatr Gastroenterol Nutr. 2017;64(4):624-31.
6.Roman Riechmann E, et al. Nutr Hosp. 2020;37(4):698-706.
7.Vandenplas Y, et al. Nutrients. 2022, 14, 530
8.Nowak-Wegrzyn A, et al. Nutrients. 2019;11:1447.
9.Boulangé CL, et al. Int. J. Mol. Sci. 2023, 24, 11422.
10.Gold MS, et al. Nutrients. 2022, 14, 2297.
HMO are not sensitive to heat. They also resist cold and are not affected by pasteurization and freeze-drying.1
1. Vandenplas Y, et al. Nutrients. 2018;10(9):1161.
No, HMO are specific to human breastmilk (hence the name, human milk oligosaccharides). Domesticated farm animals (e.g., cows) also contain “milk oligosaccharides” (MO). Human milk contains 100 to 1000 times more MO than that found in milk from domesticated farm animals, including bovine milk oligosaccharides in cow’s milk.1,2
Furthermore, MO present in milks from farm animals are qualitatively different from those in human milk. They have a higher proportion of sialylated and a lower proportion of fucosylated MO.3
1.Walsh C, et al. J Funct Foods. 2020;72:104074
2.Donovan SM, & Comstock SS. Ann Nutr Metab. 2016;69(Suppl 2):42-51.
3.Oliveira D, et al. Int J Dairy Technol. 2015;68(3), 305-21.
2’-FL and LNnT in Nestlé infant formulas are structurally identical to those found in breastmilk.1
For decades, Nestlé has studied HMO and production has recently become technically feasible. Our range of specialty formulas, Althéra® HMO, Alfaré® HMO, Alfamino® HMO and Alfamino® Junior HMO are the first to be supplemented with both 2’-FL and LNnT.
1.EC No 258/97. EFSA J 2015;13(7):4183.
The aim of adding structured lipids to Alfamino® HMO and Alfamino® Junior HMO was to mimic the composition and structure of palmitic acid in breastmilk (at the sn-2 position), which has been shown to facilitate fat and calcium absorption.1,2 Human milk is comprised of 20 to 30% palmitic acid, with 70% at the sn-2 position.3 Increasing the proportion of sn-2 palmitate in formula resulted in higher bone mineral content, reduced stool soap fatty acids, and produced softer stools more like those of breastfed infants.4 Structured lipids are triacylglycerols that have been modified to change the fatty acid composition and/or their positional distribution in the glycerol backbone.5,6
Structured lipids in Alfamino® HMO and Alfamino® Junior HMO are different from palm olein oil (found in vegetable oil-based formulas), where the palmitic acid is located at sn-1 and sn-3 positions.7
1.Delplanque B, et al. J Pediatr Gastroenterol Nutr. 2015;61(1):8-17.
2.Mazzocchi A, et al. Nutrients. 2018;10(5):567.
3.Innis SM, et al. J Nutr. 1995;125(1):73-81.
4.Kennedy K, et al. Am J Clin Nutr. 1999;70:920-7
5.Babayan VK. Lipids. 1987; 22: 417-20.
6.Osborn HT, & Akoh CC. Compr Rev Food Sci Food Saf. 2002;1(3):110-20.
7.Fabiana FY, et al. PLEFA 2013; 89 (2013) 139–143.
Tailored Solutions* with Immune Nurturing Benefits
Our tailor-made solutions include Althéra® HMO, Alfaré® HMO, Alfamino® HMO and Alfamino® Junior HMO.
*Food for Medical Purposes to be used under medical supervision
Althéra® HMO
From birth onwards.

Alfaré® HMO
From birth onwards.

Alfamino® Junior HMO